CASE STUDY 1
ACUTE LEUKEMIA PRESENTING WITH ORAL SYMPTOMS
|
A 20 years old female patient came to the institute seeking treatment for decayed teeth and bleeding gums. The complaint of bleeding gums was present for 1 month. The bleeding was spontaneous in nature and was gradually getting worse. Other symptoms were : excessive hemorrhage during menses and purple spots on the skin.
|
 |

|
|
| General examination: | |||
|
1. Conscious, co-operative patient with average built 2. Purpuric spots, about 1 to 5 mm in diameter (petechiae & ecchymoses), on the skin of the right upper chest and right forearm 3. Mild koilonychia and pallor of nail beds and conjunctivae 4. Yellowish tinge of the facial skin 5. Left submandibular lymphadenopathy.
|
|||
| Intra-oral & radiographic examination: | |||
|
Intra-oral examination of the patient showed : 1. Fully erupted complete compliment of permanent teeth. A few shallow class I carious lesions were noted. Maxillary third molars were buccally placed. The gingivae appeared healthy but spontaneous bleeding and clotted blood was noted at several margins and papillae, both buccally as well as lingually. 2. A large ulcer with irregular borders was noticed on the retromolar mucosa of the left side. A large blood clot was seen at the lateral end. The ulcer margins were dotted with petechiae. Floor of the ulcer was covered with necrotic tissue and the base was tender. A healed ulcer was seen on the right retromolar mucosa. Both ulcers were thought to be traumatic in nature; due to buccally placed maxillary third molars. 3. Purpuric spots, about 1 to 5 mm in diameter (petechiae & ecchymoses), were seen on all the mucosae. The mucosa generally appeared pale, and perhaps even yellow-tinged at places. A panoramic radiograph showed no abnormality. |
|||
 |
 |
 |
|
|
|
|
| Provisional diagnosis & investigations: | ||
|
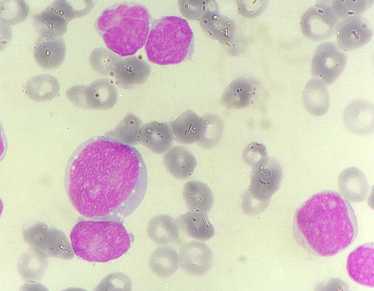
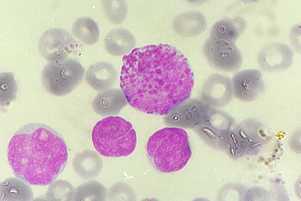
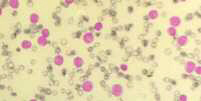
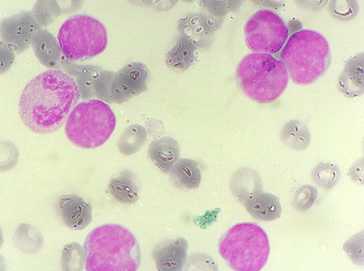
A provisional diagnosis of a bleeding diathesis, most probably a platelet deficiency or dysfunction, was made. Accordingly, blood investigations were advised. The preliminary report was suggestive of acute leukemia ! Patient was referred to a pathologist for confirmation and more specific diagnosis. The hematology report showed : Hb = 4.6 gm%; PCV = 16%; ESR = 57 mm after 1 hour; Total leukocytes = 53,000 /cmm; Reticulocyte count = 1.8% Bleeding time = 32 minutes, 30 seconds Differential leukocyte count : Myeloblasts = 92%; Neutrophils = 5%; Monocytes = 2%; Eosinophils = 1% The peripheral smear report read : "RBCs show mild to moderate anisocytosis. Majority of the cells are Normocytes. There is marked hypochromia. No immature cells. No inclusions. No parasites. WBCs are increased in number. Majority of cells are myeloblasts. Some of the myeloblasts show monocytoid differentiation. Platelets are decreased". |
||



|
|
 |
 |
 |
 |
 |
| Moral of the story: |
|
Common oral symptoms may be pointers to serious systemic disease. Presence of symptoms and signs elsewhere in the body should alert the clinician for further investigations. It is better to suspect and be proven wrong than not to suspect at all !! |
| Top |